
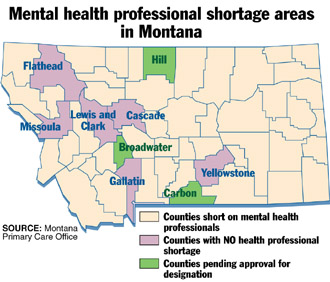
Forty-five percent of Montana's population lives in areas short on mental health care professionals. That's 397,000 people living in communities without psychiatrists or adequate numbers of other mental health care professionals, according to federal Department of Health and Human Services standards and population estimates from the U.S. Census Bureau.
 Solutions to the shortage are complicated by the limited number of psychiatrists and other health professionals, limited reimbursement for their services and special challenges of living in rural communities.
Solutions to the shortage are complicated by the limited number of psychiatrists and other health professionals, limited reimbursement for their services and special challenges of living in rural communities.
The shortage of health care professionals in rural Montana and throughout rural America doesn't end with the lack of mental health care providers. The National Health Service Corps, a federal agency that works to get health care professionals into shortage areas, reports that 45 million Americans live in communities without doctors or other medical practitioners to deliver primary health care.
In Montana, primary care providers, such as family doctors, deliver mental health care, too. But many Montanans live in counties that have been designated short of primary care doctors as well as mental health care professionals. If an area has fewer than one primary care doctor for each 3,500 residents, it is considered a primary care health professional shortage area under federal guidelines, according to Marge Levine of the state Primary Care Office in Helena.
There's a long list of Montana counties that are counted as short on primary care providers (family doctors, internists and general practitioners ) – Big Horn, Blaine, Broadwater, Carter, Daniels, Fallon, Garfield, Glacier, Granite, Hill, Judith Basin, McCone, Musselshell, Park, Petroleum, Phillips, Pondera, Powder River, Powell, Prairie, Rosebud, Treasure and Wibaux. In addition, portions of 14 other counties are short of primary care professionals. Those are: Carbon, Chouteau, Custer, Gallatin, Lewis & Clark, Lincoln, Madison, Mineral, Missoula, Richland, Roosevelt, Sanders, Teton and Toole.
Mental health professional shortage areas are determined by the ratio of psychiatrists to population. If the number of psychiatrists is less that one to 30,000, the area is considered short of mental health professionals, Levine said. Forty-seven Montana counties meet that shortage definition and three more – Broadwater, Carbon and Hill – have applications pending for mental health professional shortage status. Only the state's six most populous counties – Cascade, Gallatin, Flathead, Lewis & Clark, Missoula and Yellowstone – are deemed to have adequate numbers of mental health professionals.
What benefit is there to the time and paperwork that goes into getting a HPSA designation?
More than 30 federal programs consider health professional shortage area status in determining how to allocate grants or reimbursements for health care, Levine said. For example, doctors practicing in shortage areas receive a 10 percent premium in Medicare reimbursements. New this spring are rules for Medicare to pay for some medical specialist consultations by telemedicine, but only if the patient is in a HPSA. Also, federally-recognized rural health clinics serving health professional shortage areas qualify for Medicare payments based on their costs rather on a national fee formula.
Being a designated HPSA can bring some help, but for many communities, the help falls short of the need.
"The supply and demand are really out of reach," said Dave Young, director of the Montana Office of Rural Health in Bozeman.
One of the best benefits of HPSA status is being eligible for National Health Service Corps placements. That means doctors and other health care professionals whose medical education was financed by NHSC can practice in a health professional shortage area and work off their educational debts over a period of years. There aren't enough NHSC professionals to work in all the HPSA communities. Only five NHSC mental health professionals are working in Montana: Two social workers in Butte, one each in Libby and Ronan and a psychiatrist in Havre. Positions for a psychologist at the Great Falls mental health center and a social worker at the Missoula mental health center are pending, Levine said. The federal 2001 budget set by Congress this fall will determine whether those two positions receive funding.
Openings for one psychiatrist and one mental health therapist in Butte were listed this past week with the Montana Area Health Education Center in Bozeman, which posts help wanted notices on its Internet site. All of the vacancies reported to AHEC are in rural communities, according to Sharon Kott, who maintains the Web site. In addition to a few mental health openings, rural Montana communities last month had listed 28 openings for family doctors, internists, obstetrician-gynecologists and pediatricians.
Kott and Young agreed that it's not unusual for rural doctors to quit in less than two years. Compensation, heavy workload, having few days off, burnout and lack of employment opportunities for their spouses are among the factors that contribute to rural professional turnover, Young said.
Even professionals placed through NHSC sometimes leave after their scholarship obligation is completed. Nationally, NHSC reports, two-thirds of its professionals stay in under-served communities after completing their service requirement.
Recruiting professionals to Montana, especially Eastern Montana, is a big challenge. But an even bigger challenge for mental health professionals is generating the payments to keep them in the community. The communities of Lewistown, Glasgow and Sidney aren't recruiting psychiatrists, but local doctors and hospital administrators said they recognize a need for psychiatrists to treat patients in their towns.
There's no lack of work; there's lack of reimbursement, said Randy Holom, chief executive officer for Frances Mahon Deaconess Hospital in Glasgow. Holom noted that many of the patients in need of extensive psychiatric care rely on government health programs, such as Medicaid and the state Mental Health Service Plan.
Those programs don't cover the cost of care, according to Bob Ross, executive director of the Mental Health Center, which serves Yellowstone and 12 other south central Montana counties.
"We need a 25 percent increase in psychiatrists' pay," Ross said. "There's no reimbursement for psychiatric nursing. The doctors need psychiatric nurses to care for patients efficiently. There's no incentive for anybody to provide the service."
Montana Medicaid pays the Mental Health Center about 50 percent of what it bills, Ross said. The center's full fee for a psychiatrist's service, which includes all nursing and office services, is $150 an hour. Ross figures the actual cost of employing a psychiatrist, psychiatric nurse and receptionist is $130 an hour. But he said that the team is hard-pressed to generate that amount of revenue per hour because reimbursement is low.
For example, the state pays $71.32 for an initial psychiatric interview for purpose of diagnosing an illness. But a psychiatric evaluation may take more than an hour to complete, so it's a money-losing service, Ross said.
Early this year, the state Addictive and Mental Disorders Division promised mental health care providers a "frontier differential," a premium ranging from 20 percent to 25 percent on what Medicaid and the state's non-Medicaid mental health plan paid for some services in sparsely populated areas. The rationale for such a rural differential was that low patient volumes made it more expensive to deliver each unit of service in rural areas. If payments aren't covering providers' expenses, there may not be any services available for people who are poor and mentally ill in sparsely-populated communities.
This plan to beef up rural county payments has yet to be implemented, but "it is still in the works," Dan Anderson, administrator of the Addictive and Mental Disorders Division, said this week from Helena. For several months now, the state and its claims processing contractor have been working out the technical details of paying a different rate based on the county in which service is delivered. Anderson wouldn't predict when the higher frontier payments actually will be made. But he reiterated that the change will be retroactive to Jan. 1.
Anderson said AMDD will move ahead with its promise to beef up payments for frontier county services even though it is struggling with budget deficit estimated to be $3.6 million for the year. The division staff has begun discussing options for cutting payments. No payment increases are on the option list.
"What it boils down to is whether there will continue to be services in these frontier counties," Anderson said.
Used with permission of the Billings Gazette, copyright 2000

Please sign up below for important news about the work of The Carter Center and special event invitations.